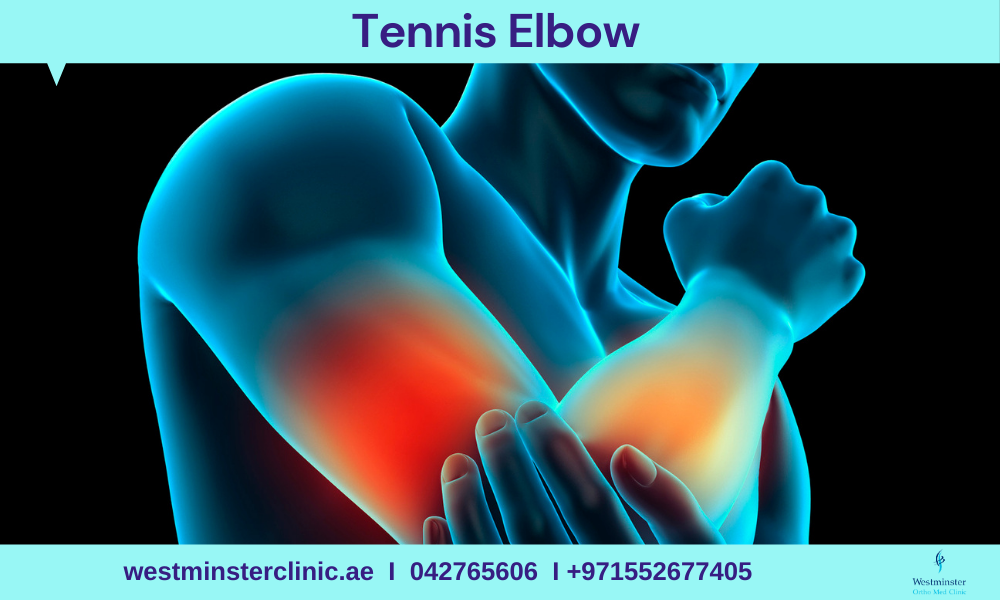
Tennis elbow, or lateral epicondylitis, is a painful condition of the elbow caused by overuse. Not surprisingly, playing tennis or other racquet sports can cause this condition. However, several other sports and activities besides sports can also put you at risk.
Tennis elbow is inflammation or, in some cases, microtearing of the tendons that join the forearm muscles on the outside of the elbow. The forearm muscles and tendons become damaged from overuse — repeating the same motions again and again. This leads to pain and tenderness on the outside of the elbow.
Causes of Tennis Elbow
Tennis elbow usually develops over time. Repetitive motions — like gripping a racket during a swing — can strain the muscles and put too much stress on the tendons. That constant tugging can eventually cause microscopic tears in the tissue.
Tennis elbow might result from:
- Tennis
- Racquetball
- Squash
- Fencing
- Weight lifting
It can also affect people with jobs or hobbies that require repetitive arm movements or gripping such as:
- Carpentry
- Typing
- Painting
- Raking
- Knitting
Risk factors
Factors that may increase your risk of tennis elbow include:
- Age. While tennis elbow affects people of all ages, it’s most common in adults between the ages of 30 and 50.
- Occupation. People who have jobs that involve repetitive motions of the wrist and arm are more likely to develop tennis elbow. Examples include plumbers, painters, carpenters, butchers and cooks.
- Certain sports. Participating in racket sports increases your risk of tennis elbow, especially if you employ poor stroke technique.
Symptoms of Tennis Elbow
The symptoms of tennis elbow include pain and tenderness in the bony knob on the outside of your elbow. This knob is where the injured tendons connect to the bone. The pain may also radiate into the upper or lower arm. Although the damage is in the elbow, you’re likely to hurt when doing things with your hands.
Tennis elbow is similar to another condition called golfer’s elbow, which affects the tendons on the inside of the elbow.
Tennis Elbow Treatment
Your doctor will first tell you to stop playing sports or doing certain kinds of work so your arm can rest. They’ll probably recommend physical therapy and some medications .
Your doctor will give you:
- Corticosteroid medications. They’ll inject these into the area to help with swelling and pain.
- A splint or brace. You’ll wear this on your arm to help your muscles and tendons rest.
- Medications. Acetaminophen or anti-inflammatory medications may be taken to help reduce pain and swelling
- Physical therapy. Specific exercises are helpful for strengthening the muscles of the forearm. Your therapist may also perform ultrasound, ice massage, or muscle-stimulating techniques to improve muscle healing.
- Ultrasound. This treatment can break up scar tissue, increase blood flow, and promote healing.
- Brace. Using a brace centered over the back of your forearm may also help relieve symptoms of tennis elbow. This can reduce symptoms by resting the muscles and tendons.
- Steroid injections. Steroids, such as cortisone, are very effective anti-inflammatory medicines. Your doctor may decide to inject the painful area around your lateral epicondyle with a steroid to relieve your symptoms.
- Platelet-rich plasma. Platelet-rich plasma (PRP) is a biological treatment designed to improve the biologic environment of the tissue. This involves obtaining a small sample of blood from the arm and centrifuging it (spinning it) to obtain platelets from the solution. Platelets are known for their high concentration of growth factors, which can be injected into the affected area. While some studies about the effectiveness of PRP have been inconclusive, others have shown promising results.
Up to 95% of people who have tennis elbow get better without surgery. But you might need it if you still have pain after 6 to 12 months. Your doctor can remove damaged tissue through cuts in your arm.
Tennis Elbow Prevention
Some small changes might help lower your risk of tennis elbow.
- Keep your arms and wrists strong and flexible. Build strength with light weights. Warm up and stretch before any activity, especially one that involves making the same motions over and over.
- Try not to make repetitive movements.
- If you play a sport with a racquet, have an expert check your equipment to be sure it’s the right size and fit.
To reduce the risk of tennis elbow, it is important to pay attention to movement techniques during exercise or exertion.
It is better to spread the load to the larger muscles of the shoulder and upper arm, rather than focus activity on the smaller muscles in the wrist and the elbow.
Warming up: Warming up before playing a sport that involves repetitive arm movements, such as tennis or squash, is essential. Gently stretching the arm muscles will help to avoid injury.
Using lightweight tools: Lighter sports equipment or racquets with a larger grip size will help reduce strain on the tendons. Damp tennis balls and older balls load the arm with unnecessary force.
Increasing the strength of forearm muscles: This can help support arm movement and prevent tennis elbow.
A physical therapist can also recommend suitable exercises to help strengthen the appropriate muscles.
Should you require additional information or would like to make an appointment with our Consultant Orthopedic Surgeon Dr. Ishrat Khan OR Physical Therapists, Anil Daniel, OR Hadel Radwan please call us or e-mail us at info@westminsterclinic.ae
Reference:
- oxfordhealth.nhs.uk
- yourphysio.org.uk
- Mayoclinic.org
Disclaimer: All contents on this site are for general information and in no circumstances information be substituted for professional advice from the relevant healthcare professional, Writer does not take responsibility of any damage done by the misuse or use of the information.